Get full access with a free account
Benefits of the Coloplast® Professional Educational platform
- Get full access to all educational content, events and resources
- Track your progress
- Share content with your collegues
- Share supporting material with your patient
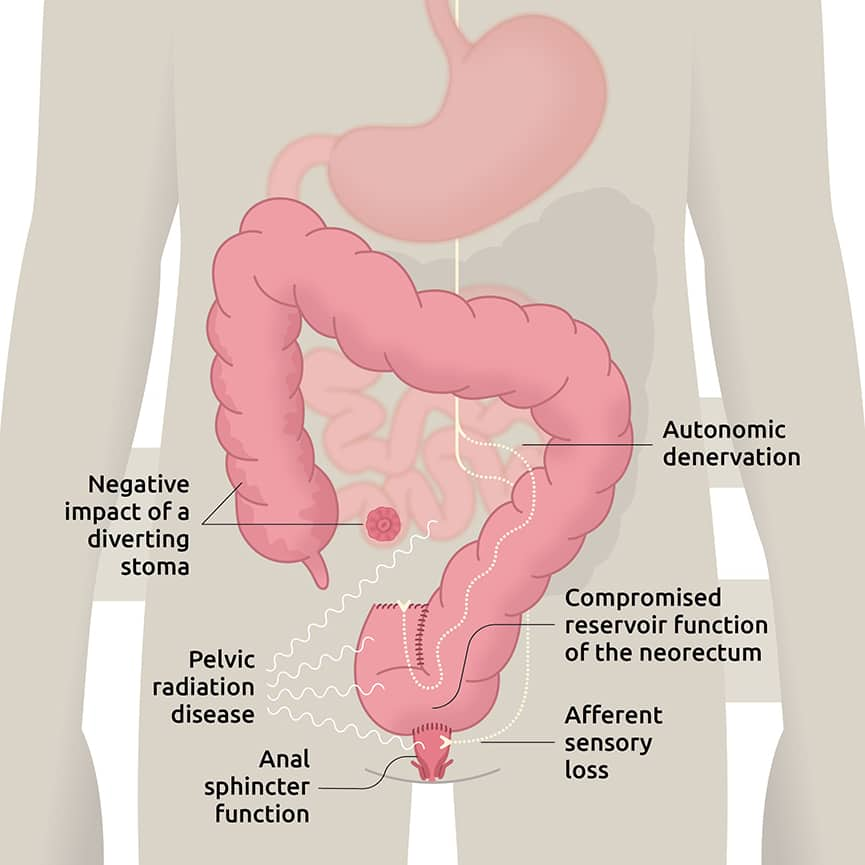
Pathophysiology
Surgical resection of the rectum and the compromised physiologic properties of the neorectum are thought to be the primary cause of LARS, due to change of reservoir function and impaired evacuation.1, 2 The length of the rectal remnant correlates with better functional outcomes, but this beneficial effect is lost in patients who received prior neoadjuvant therapy.3 Afferent sensory loss leads to diminished gas-stool discrimination and may cause frequent toilet visits.4 A temporary stoma that is used to avoid anastomotic leak after surgery may also increase the risk of LARS, although the data is conflicting.5-7 Denervation of parasympathetic and sympathetic input increases motility in the proximal colon and interrupts feedback signals in the distal colon that regulate transit.8